Septorhinoplasty in Turkey is a combined surgical procedure that simultaneously corrects nasal septum deviation and improves the external shape of the nose. It aims to enhance breathing function while achieving facial harmony. The operation is performed by ENT or plastic surgeons under sterile hospital conditions.
Cost of septorhinoplasty in Turkey is generally more accessible compared with many European and North American countries while maintaining internationally recognized medical standards. Accredited hospitals, modern surgical technologies, and experienced surgeons contribute to consistent clinical outcomes.
Recovery process after septorhinoplasty in Turkey typically includes an early healing period of one to two weeks, during which swelling and mild bruising gradually decrease. Patients are advised to follow postoperative care instructions, avoid trauma to the nose, and attend scheduled medical follow-ups.
Medical tourism for septorhinoplasty in Turkey has grown significantly due to specialized surgeons, comprehensive patient care, and integrated treatment packages. Many clinics provide preoperative assessment, surgical planning, postoperative monitoring, and coordinated accommodation services.

About Me
Prof. Dr. Fehmi Döner
ENT and Head & Neck Surgery Specialist
I completed my primary and secondary education in İzmir. I completed my medical education at Istanbul University Cerrahpaşa Faculty of Medicine in 1988. I received my specialization training at Atatürk University Faculty of Medicine, Department of Otorhinolaryngology. During my specialization training, in order to increase my knowledge and experience, I spent different periods of time at Istanbul University Istanbul Faculty of Medicine, Department of Otorhinolaryngology, and participated in clinical studies.
After receiving my specialization in 1994, I worked at Kütahya State Hospital for eight months, and then in December 1994, I was appointed as an assistant professor to the Department of Otorhinolaryngology at Süleyman Demirel University.
View MoreHow Does Septorhinoplasty Surgery Combine Aesthetics and Function?
A large portion of the patients who apply to my clinic come either only with the complaint of not being able to breathe or only stating that they are not satisfied with the shape of their nose. However, when they sit in the examination chair, we often see that these two problems are actually intertwined. This is exactly where septorhinoplasty comes into play. You can think of this surgery as both reinforcing a building’s foundation and modernizing its exterior facade. No matter how beautifully the exterior of a building with a faulty foundation is painted, cracks are inevitable over time. Likewise, correcting only the outside of a nose that is blocked inside and has weak cartilage support leads in the long term to deformities and increased shortness of breath.
The nose is the most characteristic organ located in the very center of the face and determines your expression. But at the same time, it is a tremendous air conditioner that determines the quality of every breath we take by warming, humidifying, and cleaning the air. In septorhinoplasty surgery, we surgeons apply the concept we call “functional aesthetics.” In other words, while removing a hump or lifting the tip, we also widen the air tunnels inside and correct the walls that obstruct airflow. This approach aims that when you get up from the operating table, not only your image in the mirror but also your sleep, sports performance, and overall life energy will change.
By What Mechanism Does Septal Deviation Disrupt Respiratory Physiology?
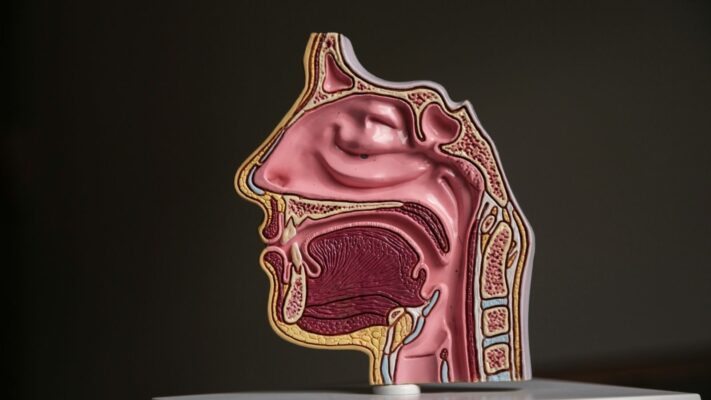
We call the structure that divides the inside of our nose into two, like a wall separating the rooms of a house, the “septum.” This wall, whose front part consists of elastic cartilage and the back part of hard bone, should ideally stand exactly in the middle. However, due to our genetic heritage, birth traumas, or falls and bumps in childhood, this wall is not perfectly straight in most of us. This curvature, which we call “septal deviation,” narrows one side of the nose while widening the other.
The physics of airflow becomes very interesting here. There is a rule of physics called the Bernoulli principle; when a fluid passes through a narrow place, its speed increases, but the pressure it applies to the walls decreases. You can think of it like a garden hose with the tip squeezed. The water spurts faster, but the pressure inside the hose drops. If you have septal deviation in your nose, the air accelerates as it passes through that narrow gap and, with the vacuum effect created, pulls your nasal wings inward. Especially when you try to take a deep breath or when running, you feel your nasal wings closing. We call this “valve collapse.” That is why correcting only the bone inside is not enough; we also need to strengthen the cartilages that support the nasal wings so that your nose does not collapse when you take a deep breath into your lungs.
What Is the Role of Conchal Hypertrophy and Nasal Turbinates in Surgery?
Another player that is often overlooked in patients with septal deviation but directly affects our surgical success is the nasal turbinates. These structures, medically called the “inferior turbinate,” are located on the side walls of the nose and are spongy tissues filled with blood vessels. Their duty is to warm and humidify the air we breathe before it goes to the lungs. The balance mechanism in our body works in an interesting way here.
When the septum deviates to one side, the airway on that side narrows. However, on the other side, a space wider than it should be forms. The body realizes that the air passing through this wide space will not be warmed sufficiently and will dry out. To compensate for this, it tries to fill that space by swelling (hypertrophy) the turbinate on the wide side. So one side becomes blocked due to bone curvature, and the other side due to swollen turbinate. If we correct only the deviated bone during surgery and bring it to the midline, then the swollen turbinate can completely block the passage in its new position. Therefore, an indispensable part of septorhinoplasty surgeries is intervening on the turbinates. With radiofrequency or tissue reduction methods, we bring these tissues to their ideal size without impairing their functions.
Is the Gender Factor Effective in Facial Analysis and Aesthetic Planning?
The biggest misconception in aesthetic surgery is the idea that there is a “one-size-fits-all ideal nose.” Yet every face has a different story, proportions, and character. In the planning we do before surgery, we analyze the patient’s face millimetrically. Forehead width, chin tip position, lip structure, and cheekbones are reference points that determine the shape of the nose we will create. Here, universal aesthetic rules called the “Golden Ratio” come into play, but the most critical determining factor is gender.
Male and female anatomy and aesthetic perception are completely different from each other. A delicate, slightly curved nose with an upturned tip that suits a woman very well can create an extremely artificial and feminine expression when applied to a man’s face. In the male nose, we aim for the dorsum to descend more straight and for the angle between the nose and the lip to be around 90 degrees. This gives the man a more charismatic and strong expression. In women, having this angle between 100–110 degrees makes the nose look slightly upturned and increases elegance in the face. In addition, the point where the nasal root starts from the forehead also affects the depth of the gaze. Our goal is not for people to say “your nose looks so nice,” but for them to say “what a beautiful expression your face has.”
Some basic parameters we consider in the preoperative analysis are as follows:
- Skin thickness
- Cartilage strength
- Chin tip position
- Forehead width
- Lip structure
- Nasal root depth
- Facial asymmetry
Contact us to get information about treatments and create an appointment!
Should Open Technique or Closed Technique Septorhinoplasty Be Preferred?
The issue my patients ask most frequently and the one that causes the most confusion on the internet is which technique the surgery will be performed with. Is the open technique better, or the closed technique? There is no single correct answer to this question; there is the “most suitable technique for the patient”:
Open technique septorhinoplasty is the procedure of lifting the skin of the nose through a very small, inverted V-shaped incision made in the area between the two nostrils that we call the “columella.” This method allows the surgeon to see the entire skeletal structure of the nose with the naked eye. It is like opening the hood of a car and repairing the engine; you are in control of everything. Especially in patients with severe deviation, those who have had surgery before, those with an asymmetric or very low nasal tip, the open technique provides us with millimetric control. Shaping the cartilages with sutures and fixing grafts (patch cartilages) exactly where we want is more reliable in this technique.
The closed technique, on the other hand, is a method in which all incisions are made inside the nostrils, leaving no visible scar from the outside. Since the connective tissues and ligaments of the nose are less damaged, there is less loss of sensation at the nasal tip and recovery may be somewhat faster. However, the field of view is limited; the surgeon shapes the nose more by feel and with experience. Today, we also use hybrid methods that combine the advantages of both techniques. What matters is not where the incision is made, but how respectfully the cartilage and bones inside are handled.
How Does Piezo Surgery (Ultrasonic Rhinoplasty) Affect Bone Healing?
When you think of old-generation nose surgeries, you probably imagine bruised eyes and swollen faces. The main reason for this was the crude instruments such as hammers and chisels used to shape the bones. While breaking the bone, these instruments could also damage surrounding vessels and soft tissues. However, Piezo technology, which has become standard in recent years, has completely changed this process.
The Piezo device works with vibrations created by ultrasonic sound waves. The most fascinating aspect of this technology is that it is “selective.” The device cuts or rasps only hard tissues such as bone. Even if the probe in your hand accidentally touches a vessel, nerve, or nasal mucosa, the device stops working and does not harm the soft tissue. What does this mean? We can shape the bones millimetrically, like a sculptor, without breaking them.
The advantages provided by piezo surgery are as follows:
- Less bruising
- Less swelling
- Controlled incision lines
- Fast recovery
- Soft tissue protection
- Precise shaping
Thanks to this, our patients experience a much more comfortable postoperative period and can return to social life more quickly.
How Is Nasal Dorsum Naturalness Achieved with Preservation Rhinoplasty?
In recent years, a “Preservation Rhinoplasty” trend has been blowing in the world of aesthetic surgery. In traditional methods, to correct a nasal hump, we would cut and remove the bony and cartilaginous roof. Since this disrupted the natural anatomical integrity of the nose, we would need to reconstruct the roof. In preservation rhinoplasty, however, the philosophy is completely different: “Don’t demolish, preserve.”
In this technique, we do not touch that beautiful, natural dorsum line of the nose and the way it reflects light. To get rid of the hump, we remove strips of bone and cartilage from the lower part, that is, from the base. Then we lower the entire nasal roof like an elevator (Let-down or Push-down technique). Thus, the dorsum of the nose remains original, smooth, and natural. This method yields excellent results especially for patients who have a hump but a well-structured nasal dorsum. It is almost impossible to tell that surgery was performed because those natural transitions that are the “signature” of the nose are not erased.
Which Cartilage Supports Are Used to Prevent the Nasal Tip from Drooping?
One of the biggest fears related to rhinoplasty is that the nasal tip will droop over time. Gravity, facial expressions, and the contracting force created by the skin during healing try to pull the nose downward. If we do not build a solid skeleton during surgery, the nasal tip may sag over time, defeated by these forces. That is why modern rhinoplasty is actually a “structural engineering” job.
To maintain the form of the nose for many years, we use cartilage grafts (support pieces). One of the most important of these is the cartilage we call the “Spreader Graft,” which supports the roof of the nose and keeps the midline air tunnel open. Another vital piece is the “Strut Graft.” You can liken this to the center pole of a tent. This strong cartilage that we place inside the columella keeps the nasal tip upright against gravity.
The most ideal material for these supports is the septal cartilage we remove from inside the patient’s own nose. However, in patients who have had surgery before or whose cartilage is very weak, we need to turn to other sources. Ear cartilage is great for shaping the nasal tip with its soft and curved structure, but its load-bearing capacity is low. If serious support is needed, for example if there is collapse that we call a “saddle nose,” then we resort to costal cartilage, the body’s strongest spare parts depot.
Get in Touch!
Contact us to get information about treatments and create an appointment!
What Are the Recovery Process and Care Recommendations After Septorhinoplasty?
The surgery is over, you have gone up to your room. So what awaits you now? First of all, we no longer see patients like in old movies, with eyes completely closed and faces wrapped. There will be a thermoplastic splint on your nose that ensures the bones fuse, and silicone splints inside your nose that allow you to breathe. Yes, you heard correctly; we no longer use meters-long gauze packing. Thanks to grooved silicone splints, you can breathe immediately after surgery. These silicone splints both accelerate healing and do not cause pain when removed because they do not adhere to tissue.
The first 48 hours are the period when swelling is most intense. During this process, it is very important to keep your head elevated and apply ice intermittently. Do not worry about pain; most of our patients talk about a feeling of fullness as if they had the flu rather than pain. Simple painkillers are more than sufficient in this period. At the end of the first week, when you come to my office, we remove the splint on the outside and the silicone splints inside. This is the moment you regain your freedom. When you first see your nose, you may find it somewhat swollen; this is very normal. The nasal skin is trying to adapt to the new skeleton underneath.
Things you should pay attention to during the recovery process are as follows:
- Risk of impact
- Use of glasses
- Heavy sports
- Extremely hot environments
- Sunlight
- Blowing the nose
70% of the swelling resolves in the first month, but for the nose to take its full shape, for the skin to thin, and for those fine details to emerge takes between 6 months and 1 year. In thick-skinned patients, this patience period is a little longer .
Why Is Revision Septorhinoplasty a More Challenging Process?
In life, we may not always achieve success on the first try. In nose surgeries, sometimes due to unpredictable behavior of healing tissue, sometimes technical inadequacies, and sometimes unfortunate traumas, a second intervention (revision) may be needed. Revision surgery is an area that requires much more experience and patience for the surgeon compared to the first surgery.
Why? Because the anatomy inside has changed, tissue planes have adhered to each other, and most importantly, the “building material” we will use to rebuild the nose, namely cartilage, has decreased. Since septal cartilage is used in the first surgery, revision procedures usually require ear or rib cartilage. However, this should not paint a pessimistic picture; with correct techniques and sufficient experience, it is definitely possible to achieve pleasing results in revision surgeries and restore both the patient’s breathing and self-confidence. What matters is that the patient’s expectations are realistic and that they trust their physician.
Latest Posts

What Is a Failed Rhinoplasty? How Does It Happen? How Is It Recognized?
Prof. Dr. Fehmi Döner » General » What Is a Failed Rhinoplasty? How Does It [...]
Read More ➜
25
Feb
Feb
Nasal Anatomy and Its Functions
Prof. Dr. Fehmi Döner » General » Nasal Anatomy and Its FunctionsNasal anatomy consists of [...]
Read More ➜
25
Feb
Feb

What Is a Nose Type and What Are the Different Nose Types?
Prof. Dr. Fehmi Döner » General » What Is a Nose Type and What Are [...]
Read More ➜
25
Feb
Feb

My Nose Is Crooked After Rhinoplasty: What Should I Do?
Prof. Dr. Fehmi Döner » Rhinoplasty » My Nose Is Crooked After Rhinoplasty: What Should [...]
Read More ➜
23
Feb
Feb

Can Asymmetry of the Nostrils Occur After Rhinoplasty?
Prof. Dr. Fehmi Döner » Rhinoplasty » Can Asymmetry of the Nostrils Occur After Rhinoplasty?Asymmetry [...]
Read More ➜
23
Feb
Feb

Nasal Massage After Rhinoplasty
Prof. Dr. Fehmi Döner » Rhinoplasty » Nasal Massage After RhinoplastyNasal massage after rhinoplasty is [...]
Read More ➜
23
Feb
Feb

Swelling on the Nasal Bridge After Rhinoplasty
Prof. Dr. Fehmi Döner » Rhinoplasty » Swelling on the Nasal Bridge After RhinoplastySwelling on [...]
Read More ➜
23
Feb
Feb

What Should Be Considered After Rhinoplasty?
Prof. Dr. Fehmi Döner » Rhinoplasty » What Should Be Considered After Rhinoplasty?What to pay [...]
Read More ➜
23
Feb
Feb