Nostril and alar base reduction surgery (alarplasty) in Turkey is a specialized rhinoplasty technique designed to decrease nostril width and refine the alar base for improved nasal symmetry. The procedure reshapes the outer nasal base through precise tissue removal, creating balanced facial proportions while preserving natural nasal function.
Alarplasty procedure in Turkey involves controlled excision of small wedges of tissue at the nostril base to narrow flared nostrils and improve nasal contour. Performed by experienced plastic surgeons, the intervention is typically conducted under local or general anesthesia and focuses on structural precision, minimal scarring, and proportional aesthetic outcomes.
Recovery after nostril and alar base reduction surgery generally progresses rapidly due to the limited surgical area and meticulous suturing techniques. Mild swelling and sensitivity may occur during the early postoperative period, while most patients resume daily activities within several days as healing advances and nasal contours gradually stabilize.
Cost and clinical standards of alarplasty in Turkey are supported by internationally accredited hospitals, modern surgical technologies, and experienced aesthetic surgeons. Treatment plans often include comprehensive consultation, operative care, and postoperative monitoring, ensuring safe procedures and predictable cosmetic results.

About Me
Prof. Dr. Fehmi Döner
ENT and Head & Neck Surgery Specialist
I completed my primary and secondary education in İzmir. I completed my medical education at Istanbul University Cerrahpaşa Faculty of Medicine in 1988. I received my specialization training at Atatürk University Faculty of Medicine, Department of Otorhinolaryngology. During my specialization training, in order to increase my knowledge and experience, I spent different periods of time at Istanbul University Istanbul Faculty of Medicine, Department of Otorhinolaryngology, and participated in clinical studies.
After receiving my specialization in 1994, I worked at Kütahya State Hospital for eight months, and then in December 1994, I was appointed as an assistant professor to the Department of Otorhinolaryngology at Süleyman Demirel University.
View MoreWhat is alarplasty and what is its role in facial aesthetics?
You have probably often heard the concept of the “golden ratio” in facial aesthetics. This ratio refers to the harmony and distances between facial structures. The width of the nasal base also plays a key role in achieving this proportion. In an ideal face, the width of the nasal wings is expected to be almost the same as the distance between the inner corners of the eyes. If the nasal wings are wider than this distance or spread excessively toward the sides of the face when smiling, the overall harmony of the face may be disrupted.
Alarplasty is a surgical intervention performed precisely at this point to reduce the width of the nasal wings (alar base), decrease the size of the nostrils, and make the curvature at the junction of the nose and cheek more aesthetic. This procedure is not merely a “cut and remove” process; on the contrary, it is the art of rearranging the architecture of the midface. Many of our nasal patients also have facial asymmetry. In other words, one side of the face is smaller, and the face and nose are inclined toward that side. In these patients, the nasal wing on the smaller side compared to the other side of the face is usually longer. By removing a certain amount from the nasal wing at the lower groove, the wing heights are also equalized. Excessively wide nasal wings can make a person look older, harsher, or more tired than they are. Narrowing this width with millimetric calculations softens the facial expression and provides a more elegant appearance.
What is the anatomical structure and function of the nasal wings?
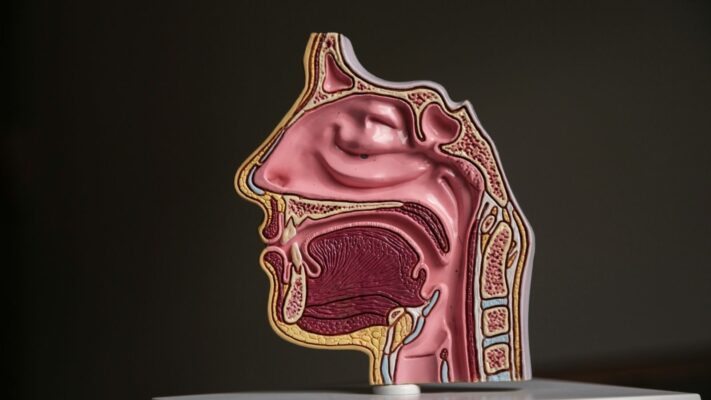
From the outside, the nasal wings may look like a simple skin fold, but in fact they contain an extremely complex and dynamic structure underneath. Seeing this area as just a piece of skin would be a major mistake. The nasal wings are intertwined with cartilage supports beneath the skin, fat pads, connective tissues, and most importantly the muscles that control our facial expressions.
The nasal base is like a bridge extending from the nasolabial groove where it meets the cheek to the column in the middle of the nostrils that we call the columella. The most important feature of this area is that it is mobile. When we smile, speak, take a deep breath, or get angry, our nasal wings move. This movement is provided by special muscle groups in the region. These muscles create facial expressions by pulling the nasal wings outward and upward. Respecting the presence of these muscles during surgery and not impairing their function is of vital importance. If one focuses only on reduction and the attachment points of the muscles are damaged, the person may have a “frozen” or “mask-like” expression after surgery. Therefore, alarplasty is not simply a tissue removal procedure; it is a procedure that provides aesthetic improvement while preserving function.
Who are suitable candidates for alarplasty and what is considered in patient selection?
As in every aesthetic procedure, proper patient selection is the key to success in alarplasty as well. This surgery may not be suitable for everyone, or everyone’s needs may be different. Individuals who are generally satisfied with the main framework of their nose (its hump or height) but are bothered by the width or shape of their nostrils are the most ideal candidates.
People who think their nostrils look too dominant relative to their face when they look in the mirror, who feel the need to constantly hide their nose when taking photos, or who think their nose spreads across their face when they smile benefit greatly from this operation. However, the most important criterion here is that the patient’s expectations are realistic. A reduction can be performed only to the extent allowed by the nasal structure; pushing the natural limits of the tissue may lead to breathing problems. In addition, smoking should definitely be evaluated before the operation and must be stopped, since it negatively affects the delicate blood circulation in this area.
Common characteristics of suitable candidates are as follows:
- Nasal wings being wide enough to exceed the facial boundaries
- Asymmetrical nostril structure
- Excessive widening of the nasal wings during smiling
- A flattened nostril base
- Deformity of the nasal wing after trauma
- Having undergone rhinoplasty before but the wings remaining wide
How is the analysis of nasal width and nostril size performed?
When evaluating a patient, focusing only on the nose can be misleading. The face is a whole, and the nose is part of that whole. In the analysis process, the patient’s face is first examined in detail from the front and in profile. Imaginary vertical lines descending from the inner corners of the eyes are a reference point for us. In an ideal aesthetic perception, the nasal wings are expected to remain between or at the borders of these lines. If the wings extend beyond these lines, we can speak of a wide nasal base.
In addition, the geometric shape of the nostril is also very important. Nostrils can have different forms such as teardrop, round, horizontal oval, or vertical oval. This shape is decisive when determining which technique will be used. Moreover, the angle at which the nasal wing attaches to the cheek, how far forward the nasal tip is (projection), and the lip structure are also included in the analysis. Sometimes, in a patient with a very low nasal tip, the nasal wings may appear wider than they actually are; in such a case, even lifting the nasal tip alone can make the wings be perceived as narrower. Therefore, during analysis, the relationship between the nose, lips, chin, and cheeks is evaluated three-dimensionally.
Contact us to get information about treatments and create an appointment!
What is the wedge excision technique and in which cases is it applied?
When alarplasty is mentioned, one of the methods most frequently used by surgeons and considered a “gold standard” is wedge excision. This technique is an excellent solution especially for cases where the nasal wings are excessively convex outward, which we call “flare.” In some patients, the inside of the nostrils is not very wide, but the outer part of the wings is very fleshy and curved. This method is preferred to correct that curved structure.
The logic of the technique is based on removing a wedge-shaped (triangular prism-like) piece of tissue from the natural fold line where the nasal wing meets the cheek. The greatest advantage of this method is that it can reduce only the outward curvature of the wing without narrowing the inner circumference of the nostril, that is, the air inlet area. Thus, while the patient’s breathing capacity is not affected, a flatter and more elegant wing structure is achieved aesthetically.
In this technique, the placement of the incision is very critical. The cut is hidden in the natural shadowed area at the junction of the nasal wing and cheek (alar-facial groove). In this way, when healing is complete, the scar disappears within this natural shadow and becomes almost impossible to notice. Wedge excision softens the appearance of the nose especially from the side profile and makes the nose-cheek transition more aesthetic.
How is the nasal base width narrowed with sill reduction?
In every patient, the problem may not be outward convexity of the wings. In some cases, the nasal wings are flat, but the base of the nostrils, that is, the floor, is very wide. In that case, the nostrils look far apart and the nasal base presents a flattened appearance. In such situations, the technique called “sill excision” comes into play. The sill is the threshold area right at the entrance of the nostril.
In this method, a geometrically calculated piece of tissue is removed from the base of the nostril. The goal is to bring the nasal wings closer together from the base. We can liken this to closing the legs of a compass; as the compass angle narrows, the legs approach each other. Sill reduction also narrows the stance angle of the nasal wings on the face. This technique is extremely effective especially in patients whose nostrils are horizontal oval and whose nostrils extend very far to the sides when they smile.
Most of the time, our patients have both wing flare and base width together. In this case, as surgeons, we apply wedge excision and sill reduction in combination. This hybrid approach corrects both the curvature of the wing and positions the nostrils ideally, thus achieving a complete aesthetic improvement.
What is the gingival approach, a scarless method, and what are its advantages?
There are certain special cases in which traditional methods, that is, removing tissue by making an incision through the skin, are not always appropriate. The medical world is constantly developing, and surgeons are in search of methods that leave fewer scars and provide more natural results. In this context, the “Gingival Approach,” developed especially with contributions of Turkish surgeons to the literature, is a remarkable technique. This method is used particularly in challenging cases that we call nasal alar retraction, where the nasal wing is pulled upward.
The biggest difference of this technique is that no incision is made on the skin from the outside. The procedure is performed entirely through the mouth. By entering from the gum line under the upper lip at the level of the canine tooth, the surgeon reaches the periosteal level beneath the nasal wing. The soft tissues and ligaments there are released, and the nasal wing that has been pulled upward or positioned abnormally due to tension is brought into its natural position.
The advantages of this method are:
- No externally visible incision scar
- Preservation of the facial expression muscles in the nasal wing
- Not disrupting the natural smile expression
- Fast recovery process
- No tissue loss
How does the surgery process proceed and how is the anesthesia method determined?
Alarplasty is a generally short and painless process in which patient comfort is prioritized. The choice of anesthesia is determined according to the scope of the procedure to be performed and the patient’s psychological state. If only the nasal wings will be addressed (isolated alarplasty), the procedure can be safely performed under local anesthesia. This is similar to getting a filling at the dentist; only the nasal area is numbed, the patient is awake, but feels no pain.
However, some of our patients may feel anxious about being aware in the operating room environment. In that case, mild sleepiness called sedation or general anesthesia may be preferred. In addition, when alarplasty is performed as part of a full rhinoplasty surgery, the procedure is carried out at the end of that process since the patient is already under general anesthesia.
The operation time for alarplasty alone averages between 45 minutes and 1 hour. Detailed drawings and measurements made before the surgery are the most important part of the process. The surgeon marks the tissue to be removed by making millimetric calculations on the patient’s face. This stage is vital for the symmetry of the result. After the procedure is completed, the incision sites are closed with very fine aesthetic sutures, and the patient can be discharged on the same day after a short observation period.
Get in Touch!
Contact us to get information about treatments and create an appointment!
What is the recovery process like and what should be considered?
One of the topics our patients are most curious about is the postoperative period. Recovery after alarplasty is much faster and easier than major nasal surgeries that involve the bones. Bruising on the face and swelling around the eyes are not expected with this surgery. Our patients generally feel quite well even immediately after the operation.
In the first 48 hours, mild edema in the nasal wings and minimal bleeding in the form of slight oozing are normal. During this period, keeping the head elevated and applying intermittent ice helps the swelling subside quickly. Pain is usually very mild and can be easily controlled with simple painkillers. The stitches are usually removed between the 5th and 7th days. Suture removal is completely painless. After the stitches are removed, the patient can fully return to social life. In some cases, when dissolvable stitches are used, there is no need for suture removal.
Things to pay attention to during the recovery process are as follows:
- Keeping the wound area clean and dry
- Applying the prescribed antibiotic creams regularly
- Avoiding heavy sports for a while
- Avoiding excessive facial expressions
- Taking a break from smoking and alcohol consumption
- Not performing forceful nose blowing
Will there be permanent scars after alarplasty and how are these scars concealed?
In rhinoplasty, the issue of “scars” is always a sensitive point. To be honest, in every procedure where the skin is cut, technically a scar forms. However, the art of surgery lies in making this scar “invisible.” Scar management in alarplasty is one of the most important indicators of surgical success.
In a successful alarplasty, incisions are not made in random locations. The natural anatomical folds of the face are perfect hiding areas for surgeons. Especially the groove between the nasal wing and the cheek is an area where light naturally creates shadow. When incisions are placed exactly within this groove, the fine line that forms after healing disappears within this shadow. Rarely, when you come very close and open the groove, a faint light line may be seen.
In addition, the suture materials and technique also determine the quality of the scar. Multi-layer closure techniques performed using materials that are much thinner than a strand of hair, without fibers, and that do not damage tissue ensure that the wound edges come together without tension. A wound without tension heals without leaving a scar. In the early stages of healing, there may be slight pinkness at the incision sites, but this gradually fades to the skin color and becomes indistinct. The patient’s genetic wound healing potential is also an important factor, but with modern techniques, the risk of a noticeable scar has been minimized.
What are the possible complications and how are risks managed?
As with every medical intervention, there are theoretically some risks in alarplasty as well. However, with an experienced surgeon and appropriate technique, these risks are quite rare. Patients being informed about this helps us manage the process more safely.
The most common issue is temporary asymmetries. The human face is usually asymmetrical by nature. In colloquial terms, we resemble seven generations and inherit genetic traits from the whole family. Because different genes come together, the bones and structures on each half of our face may not be identical mirrors of each other. Similarly, the two nostrils are never exactly the same even before surgery. Temporary asymmetries may be seen after surgery due to swelling subsiding at different rates, but this resolves as the tissues heal. The risk of infection is quite low because blood supply in the facial area is very good.
Possible risks are:
- Temporary or permanent asymmetry
- Development of infection at the wound site
- More noticeable scar than expected
- Excessive narrowing of the nostrils
- Difficulty in breathing
- Reaction to suture material
Most of these risks can be prevented with good preoperative planning and careful postoperative care. For example, the risk of excessive narrowing is eliminated when the surgeon follows the principle of “conservative surgery.” The aim is always to achieve aesthetics without impairing function.
What are the advantages of combining alarplasty with rhinoplasty?
Alarplasty can be performed alone, but it is often applied as a complementary part of a full rhinoplasty surgery. In fact, in many cases, the decision for alarplasty is made at the very end of the rhinoplasty procedure. There is a very important technical reason for this:
When the nasal tip is lifted (projection is increased) or the nasal dorsum is thinned during rhinoplasty, the nasal wings may appear visually wider or flatter due to tension. In other words, nostrils that appear normal at the beginning of the surgery may start to stand out after the nasal tip is shaped. It may not always be possible to predict this in advance. Therefore, surgeons usually complete the main procedure, give the nasal tip its final shape, and then re-evaluate the nasal wings.
If the wings still appear wide or incompatible with the face once the nasal tip has taken its new position, alarplasty is added in the same session. This holistic approach ensures that not only the profile view of the nose but also the frontal view is flawless. Performing both procedures together enables the patient to reach the full result with a single anesthesia and a single recovery period. In addition, since the nose is a whole, the proportion of the wings with the nasal tip can only be seen clearly once all structures are in place.
Does reducing the nostrils make breathing more difficult?
One of our patients’ biggest concerns is the fear that when the nostrils are reduced, the air inlet will decrease and breathing will become more difficult. This is a very valid and logical question. However, in a properly planned surgery, the answer to this question is definitely “no.”
In the physiology of breathing, the size of the air inlet area (nostril entrance) is not the only determining factor. In fact, in some cases, excessively wide or lax nasal wings can cause the wings to collapse inward due to a vacuum effect during deep breathing (nasal valve collapse). This paradoxically makes breathing more difficult. When the wings are tightened and structurally supported with alarplasty, this collapse can be prevented and breathing quality can improve.
The critical point here is that the surgeon must not damage the narrowest airway passage area inside the nose that we call the “valve.” Techniques such as wedge excision do not narrow the airway because they correct only the outer curvature without reducing the inner diameter of the nostril. In sill excision, the amount of narrowing is kept within safe limits that will not affect the airway. The surgeon’s priority is always the patient’s healthy breathing; aesthetic concerns must never take precedence over function.
Are the results permanent and how does the aging process affect the nasal structure?
The results achieved with alarplasty are permanent. The removed tissue does not grow back, and the nasal wings do not return to their former width. In this respect, alarplasty provides the patient with a lifelong aesthetic benefit. Within the first few months after surgery, as swelling subsides, the nose takes its final shape, and this shape becomes permanent.
However, it should not be forgotten that aging is a dynamic process, and like the entire face, the nose is also affected by this process. Over the years, loss of skin elasticity, the effect of gravity, and changes in soft tissues may cause minimal changes in the nasal structure. For example, the nasal tip may drop slightly with age, or the skin may thin and loosen. However, this natural process does not cause the narrowed nasal base achieved with alarplasty to widen again.
Weight changes are also a factor that can affect the result. In cases of excessive weight gain and loss, since the fat tissue in the face will change, the appearance of the nasal wings can also be indirectly affected. However, overall, alarplasty is a stable procedure that provides long-term satisfaction. Our patients remain satisfied with the harmony of their noses with their faces even years later.
Latest Posts

What Is a Failed Rhinoplasty? How Does It Happen? How Is It Recognized?
Prof. Dr. Fehmi Döner » General » What Is a Failed Rhinoplasty? How Does It [...]
Read More ➜
25
Feb
Feb
Nasal Anatomy and Its Functions
Prof. Dr. Fehmi Döner » General » Nasal Anatomy and Its FunctionsNasal anatomy consists of [...]
Read More ➜
25
Feb
Feb

What Is a Nose Type and What Are the Different Nose Types?
Prof. Dr. Fehmi Döner » General » What Is a Nose Type and What Are [...]
Read More ➜
25
Feb
Feb

My Nose Is Crooked After Rhinoplasty: What Should I Do?
Prof. Dr. Fehmi Döner » Rhinoplasty » My Nose Is Crooked After Rhinoplasty: What Should [...]
Read More ➜
23
Feb
Feb

Can Asymmetry of the Nostrils Occur After Rhinoplasty?
Prof. Dr. Fehmi Döner » Rhinoplasty » Can Asymmetry of the Nostrils Occur After Rhinoplasty?Asymmetry [...]
Read More ➜
23
Feb
Feb

Nasal Massage After Rhinoplasty
Prof. Dr. Fehmi Döner » Rhinoplasty » Nasal Massage After RhinoplastyNasal massage after rhinoplasty is [...]
Read More ➜
23
Feb
Feb

Swelling on the Nasal Bridge After Rhinoplasty
Prof. Dr. Fehmi Döner » Rhinoplasty » Swelling on the Nasal Bridge After RhinoplastySwelling on [...]
Read More ➜
23
Feb
Feb

What Should Be Considered After Rhinoplasty?
Prof. Dr. Fehmi Döner » Rhinoplasty » What Should Be Considered After Rhinoplasty?What to pay [...]
Read More ➜
23
Feb
Feb